Some stomach GISTs smaller than 2 cm may pose more risk than previously thought according to a new report from China. In this small retrospective study1 by Dr. Jianjun Yang and colleagues from Xijing Hospital of Digestive Diseases, the mitotic rate exceeded 5/50 High Power Field (HPF) in 14 of 63 cases (22.2%). Mitotic rate is used with tumor size and tumor location to determine the risk of recurrence after surgery for GIST patients. Several risk assessment methods also add tumor rupture as an additional high-risk factor. 5/50 HPF is frequently used as the dividing line between high and low risk GISTs, with most systems considering tumors of 5/50 HPF or less to be lower risk while tumors above 5/50 HPF are generally higher risk. An exception is the GIST nomogram which considers primary tumors of exactly 5/50 HPF to be of generally higher risk (a complete risk rating also depends on tumor size and location).
Current United States (NCCN) and European (ESMO) treatment guidelines allow for monitoring these tumors without surgery in some cases. For example, in the U.S., surgery is recommended for small tumors when an ultrasound (EUS) shows high-risk features2. For tumors without high-risk features, the U.S. guidelines say to “consider endoscopic surveillance at 6-12 month intervals.” They note however, that “Endoscopic ultrasonography surveillance should only be considered after a thorough discussion with the patient regarding the risks and benefits.”
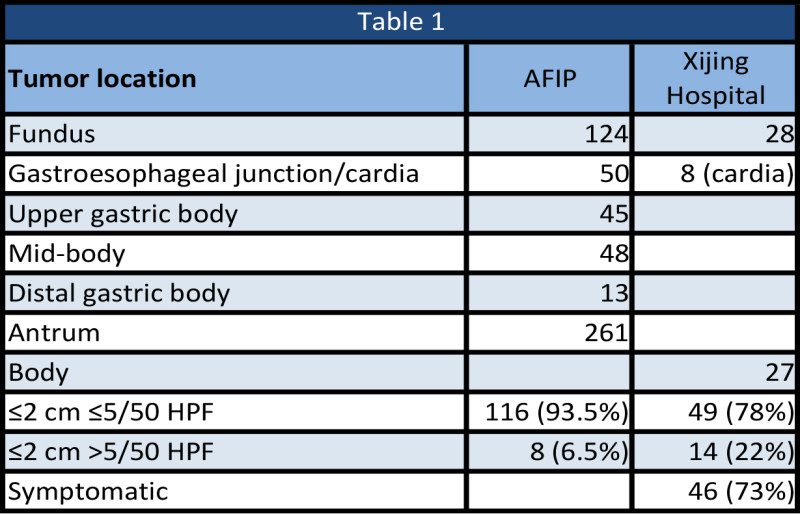
In a study of 1,765 cases of GIST stomach tumors, the Armed Forces Institute of Pathology (AFIP), found 124 cases where the primary tumor was less than or equal to 2 cm (7%). In these small stomach tumors, tumor-related mortality was essentially zero, however, only eight of these tumors had a mitotic rate greater than 5/50 HPF. There was no recurrence information available for the Yang study, so despite the higher frequency of “high-mitotic rate” tumors, the results should be interpreted with caution.
Most patients in the Yang study presented with clinical symptoms despite the small tumor size. Symptoms included pain (29%), bleeding (8%) and discomfort (37%); 27 percent were asymptomatic.
Some questions about small stomach GISTs remain. Dr. Heikki Joensuu, the principal investigator of the one year versus three year adjuvant imatinib trial, has written a brief communication to the Lancet journal about this question (due out in a few weeks). We asked Dr. Joensuu these questions:
1. How many patients with small gastric GISTs are symptomatic?
Dr. Joensuu: “This percentage depends on the size, but the great majority are unsymptomatic. The most common symptom is anemia.
2. Should symptomatic patients have surgery?
Dr. Joensuu: “-In my opinion yes, unless there are co-morbidites or risks related to surgery.”
3. Should patients with small tumors in the cardia consider surgery and/or should location within the stomach be considered when deciding on surgery
Dr. Joensuu: “I am not convinced about the location in the stomach yet. Mitotic count is probably a more important parameter.”
4. Do biopsy procedures (when surgery is not performed) used for small stomach GISTs accurately assess mitotic rate (does a needle or small sample size hit the most mitotically active part of the tumor)?
Dr. Joensuu: “I do not think mitotic count can ever be regarded accurate, since there are differences between pathologists in identification of the mitotic figures, the fields-of-views of the microscopes vary, there are sampling variations, and fixation variations. Yet, perhaps paradoxically, mitotic counting is still the best prognostic factor we have. Using a single cut-off value (5 mitoses/50 HPFs) does not make much sense, since the mitotic count is clearly a continuous variable, and prognosis does not change abruptly from good too bad at five mitoses/50 HPFs. I prefer to use the continuous scales for prognostication.”
This article pertains to small stomach tumors. Small tumors located in a different organ may have different risk criteria. In particular, high mitotic rate is more common in small rectal GISTs and many of these may have a high risk of recurrence (Miettinen et al.).
1 Yang, J. et al. Surgical resection should be taken into consideration for the treatment of small gastric gastrointestinal stromal tumors. World Journal of Surgical Oncology 11, 273 (2013)
2 Possible high-risk EUS features include irregular border, cystic spaces, ulceration, echogenic foci and heterogeneity.