The Life Raft Group has vocally supported mutational testing for many years. Countless articles have been written in prior LRG newsletters about what this testing is, how it can be beneficial to treatment, and even about trials that target a specific mutation. However, as of May 1, 2011, the LRG patient registry only received 377 reports of mutations out of 1,327 patients, which only represents 28 percent of the entire registry. Part of this may be related to the fact that mutational testing is not common practice at diagnosis, or some patients, guided by an oncologist’s care, might feel it is unnecessary to perform the test if they have been stable or disease-free for more than a few years.Regardless of the whys, we are still able to identify certain trends, even with a small population.
What we do know from the LRG’s data is that a primary mutation in the KIT gene accounts for 73 percent of this group. Of the total group 58.36 percent of these reports are patients with the KIT Exon 11 mutation. Exon 9 represents 12.47 percent of the total group and exon 13 makes up only 2.1 percent. While wildtype patients make up 17 percent of the group, we are seeing a few patients identifying their mutations as BRAF or SDH mutations. Lastly, patients with the PDGFRA mutation are comprised mostly of Exon 18, which is 6.1 percent, and the majority of Exon 18 does have the D842V mutation. We have less than two percent who have the exon 12 mutation.
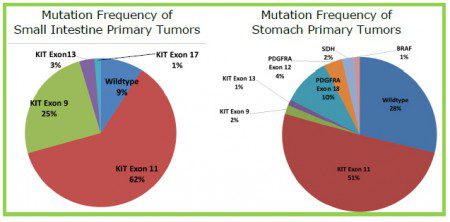
Mutations in the Stomach and Small Intestine
A common question that is asked is if a particular mutation is commonly associated with a primary tumor location. What we have seen with primary tumors located in the small intestines and the stomach is that in both locations, Exon 11 mutations appear in more than 50 percent of diagnosis. While we have received more reports of exon 9 in 25 percent of cases with a primary in the small intestines, this mutation has only appeared in two percent of cases in the stomach. The reverse is seen in wildtype mutations, where 28 percent are seen in the stomach, while only nine percent are diagnosed in the small intestines. With other rare mutations such as PDGFRA and SDH, we have not received any reports of these mutations appearing in the small intestines, but more so with primary tumors located in the stomach. However, with tumors that appear at junction points we have obtained one report of PDGFRA exon 18 appearing in the stomach and small intestine junction area. With tumors that appear at the junction of the esophagus and stomach, we have seen at least four cases with the mutation exon 11 and one with exon 9. Exon 13 mutations occurred in the small and large bowel and the rectum and not in the stomach.